The question at the heart of the red light therapy bone test is simple: can red and near-infrared light actually get through bone and reach tissues beneath, such as the brain or marrow? I set up a series of hands-on measurements to learn not just whether light passes through bone, but how much of the original energy survives the journey. The results matter if you are using red light therapy for cognitive support, hair growth, or to treat deep tissues and joints.
Why This Question Matters
The promise of red light and near-infrared therapy is powerful: improved mitochondrial function, reduced inflammation, faster recovery, and improved cognition. But those mechanisms assume photons reach target tissues. A red light therapy bone test is useful because bone is a significant optical barrier. The skull, for instance, is thicker in some regions and varies between sexes and ages, so understanding penetration informs device choice, dosing, and realistic expectations.
What I Tested and Why
I wanted a practical, measurable look at penetration. For this red light therapy bone test I used three main elements:
- a compact battery-powered red/NIR handheld emitter with dual-chip LEDs
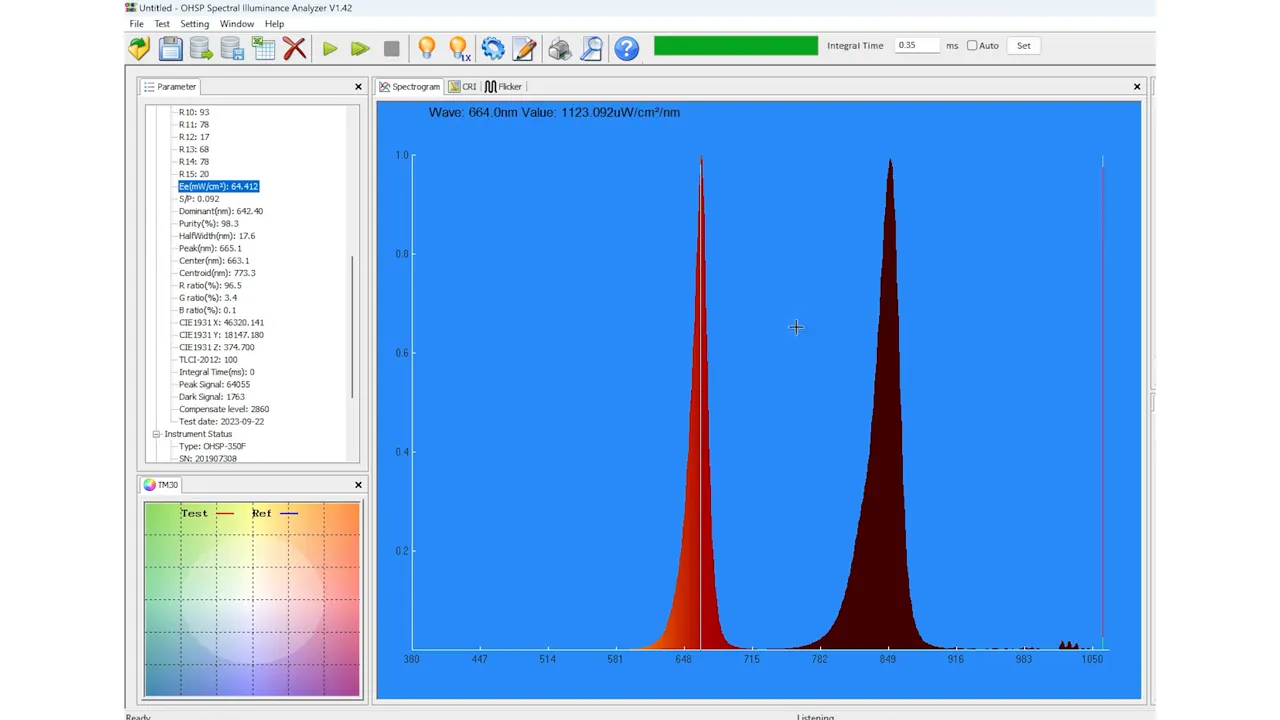
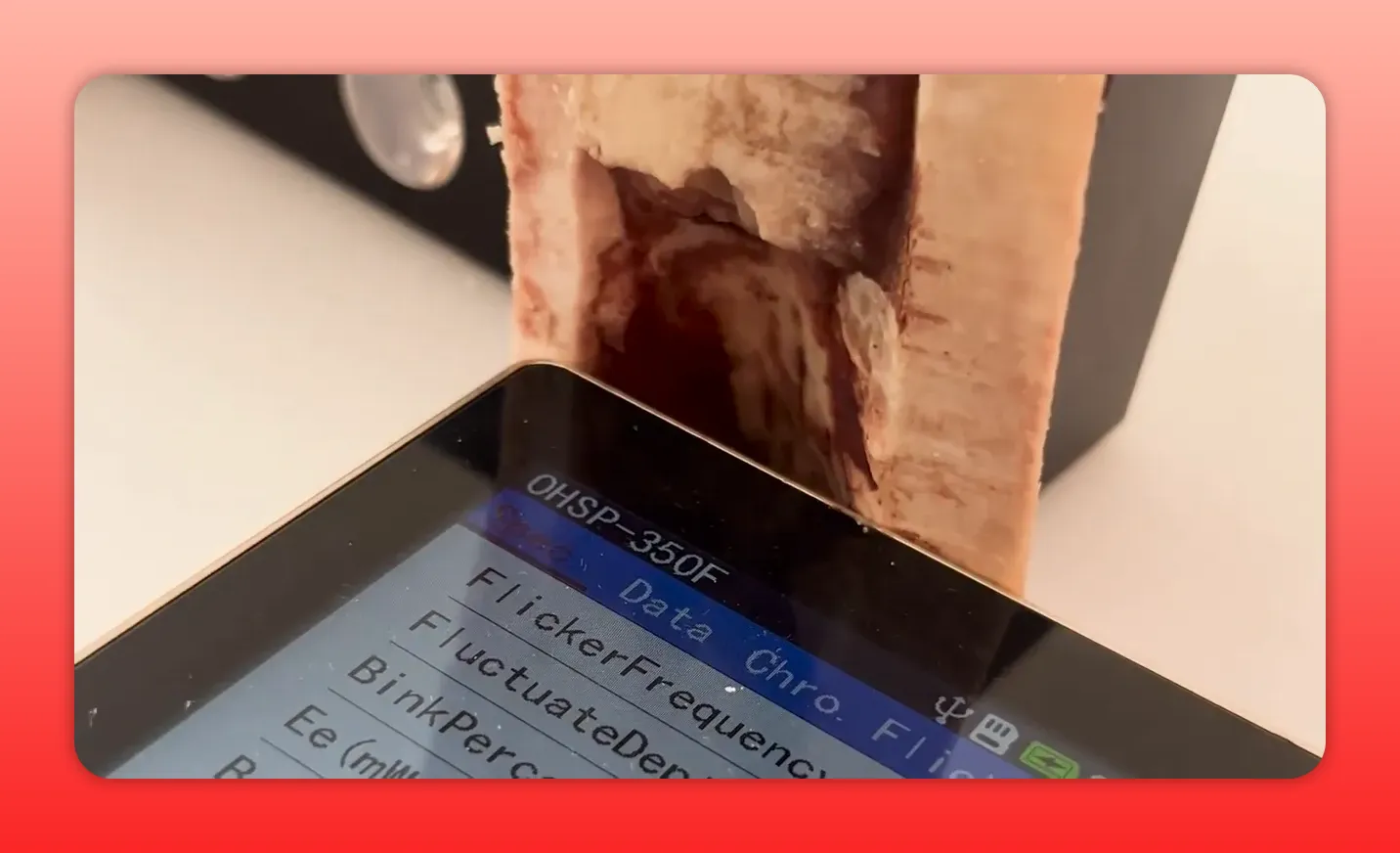
- a spectrometer to quantify radiance and spectral distribution at the sensor
- two biological specimens: a halved cow tibia (bone with and without marrow) and a cleaned goat skull
The tibia cross-section measured roughly 9–10 millimeters at its thickest point, which closely matches the thicker portions of an adult male skull. The marrow provides a fatty, brain-like medium for testing penetration through more than just mineralized bone. The goat skull is thinner but useful for visual confirmation and for seeing how light moves through sinuses and cavities.
Setup: How the Measurements Were Taken
For a clear baseline, the emitter was placed about one inch from the spectrometer sensor and recorded a spectral output with two distinct peaks: one in the red band (~660 nm) and one in the near-infrared (~850 nm). In the initial configuration the emitted energy split roughly 50/50 between red and near-infrared, and the radiance reading was around 64–65 milliwatts per square centimeter.
For the red light therapy bone test I first measured this baseline, then placed the bone between the emitter and the spectrometer and recorded the change. Measurements were repeated in several orientations and configurations: bone only, bone with marrow in place, and thin bone regions that mimic thinner cranial areas.
Tibia Bone Results: How Much Light Gets Through?
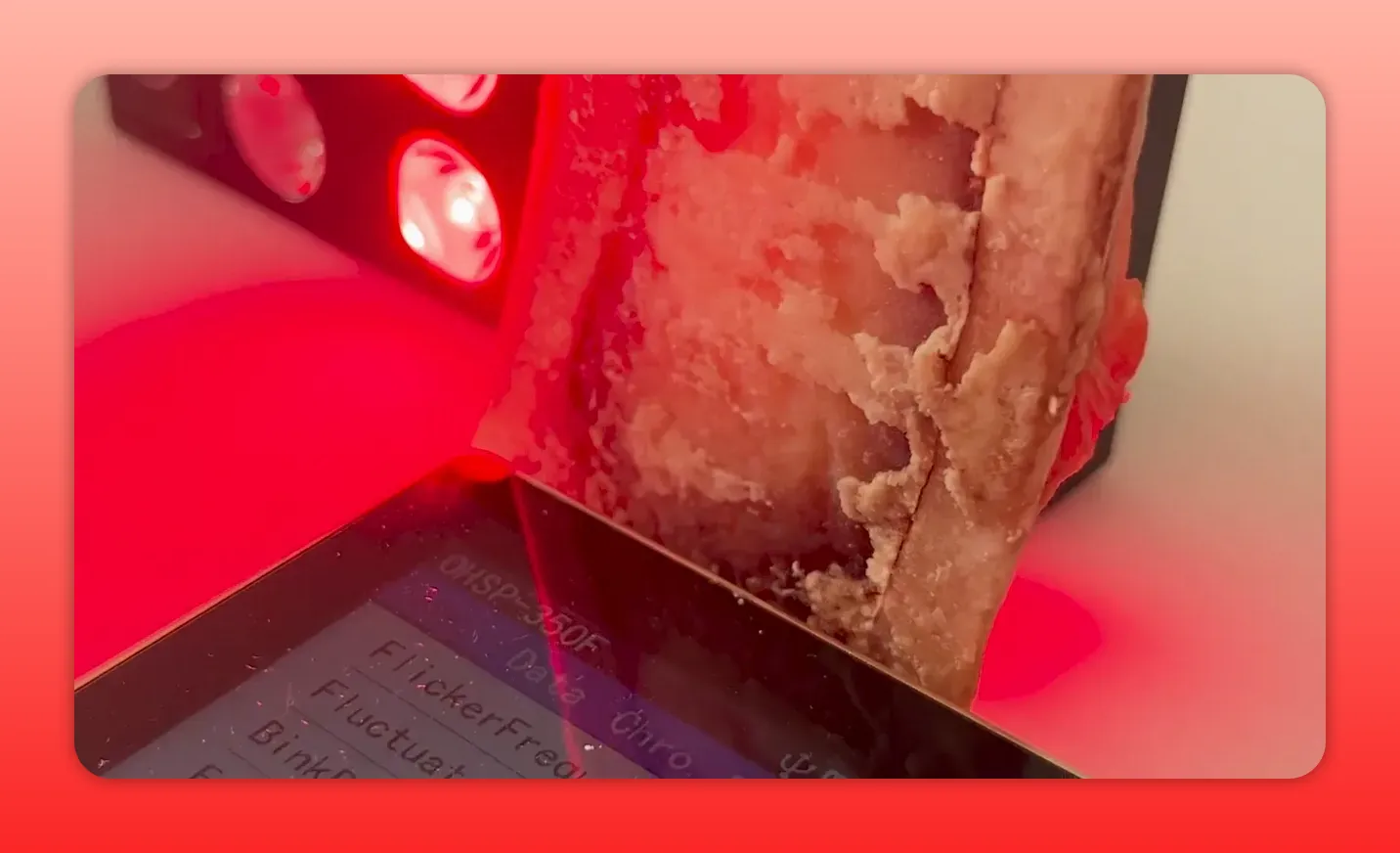
With the thick cross-section of tibia placed flush against the sensor, the spectrometer readings dropped dramatically. Radiance went from the baseline of roughly 64 milliwatts per square centimeter down to about 3.7–3.8 milliwatts per square centimeter. That means only about 6 percent of the incident light reached the sensor through roughly 9–10 millimeters of bone in this configuration.
That 94 percent reduction is significant, but important context changes the interpretation. The spectral distribution shifted toward near-infrared dominance once the bone was introduced. In other words, the near-infrared portion passed through bone far better than the red band. The spectrometer showed roughly three to four times more power in the near-infrared wavelengths on the reading that passed through the bone.
So the headline from the red light therapy bone test is twofold: bone blocks the majority of light, but near-infrared wavelengths penetrate far better than visible red.
Adding Marrow and Different Orientations
Next I ran the test with the marrow side involved and with different bone orientations. When the bone was positioned so the light traversed both mineral and marrow, the radiance values dropped even further in some setups. In one position the reading was around 0.142 milliwatts per square centimeter from a baseline near 55. That means only about 0.25 percent of incident light made it through in that specific geometry.
Other orientations—through thinner sections of bone or through bone aligned with a bright hotspot of the emitter—produced higher readings (for example, about 1.3–1.4 milliwatts per square centimeter). Thinner bone and careful alignment increased transmitted energy, as expected. The takeaway is that local thickness, composition, and angle matter. A single number is useful, but the range tells the real story.
Goat Skull Test: Seeing Light Move Through Cavities
A goat skull is not a human skull, but it provides a real demonstration of how light travels through sinuses and thin bone. The oral cavity, sinuses, and eye sockets act as windows where light can move and scatter. Placing the emitter into the jaw area made the inside glow; the spectrometer detected measurable radiance on the opposite side.
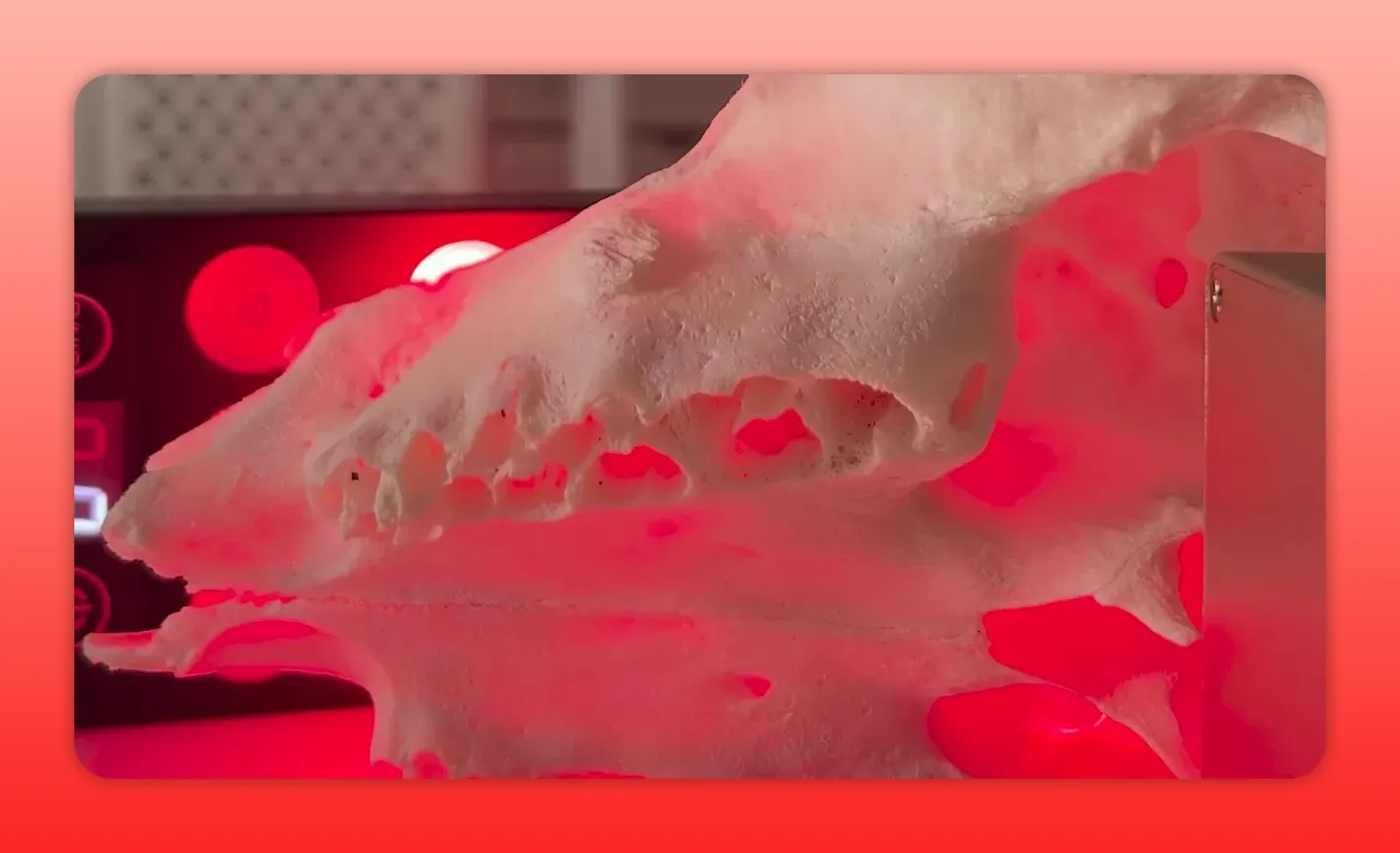
In one skull configuration I measured a baseline of about 21 milliwatts per square centimeter at the sensor, then dropped to around 0.66 milliwatts per square centimeter with the thin skull bone in place. Again, the near-infrared wavelengths were the main contributors to what got through. The red light therapy bone test with the skull shows that cavities and thinner regions allow more energy transfer and that, practically, certain anatomical windows conduct light better than thick cortical bone.

Putting the Numbers into Perspective
Here are the practical implications of those radiance numbers from the red light therapy bone test:
- If a device produces 40–80 milliwatts per square centimeter at a comfortable treatment distance (typical for quality panels measured at 6 inches), only a fraction will reach deep tissues beneath bone.
- For thick skull regions, expect single-digit milliwatts per square centimeter, often in the 1–4 mW/cm² range depending on device power and positioning.
- For thinner cranial areas or cavities, delivered energy is higher. Eyes, sinuses, and jaw openings can act as transit zones for light.
- Near-infrared wavelengths around 800–900 nm consistently outperform visible red (~660 nm) at penetrating bone and fatty tissues.
It is also worth noting that the brain likely needs less delivered optical energy than a muscle or joint to trigger biological effects. Some studies suggest neuronal tissues respond to lower fluence. That means even a reduced percentage of incident light may be biologically relevant. The red light therapy bone test shows penetration is not zero, and for many applications that is enough to produce measurable changes.
What This Means for Device Choice
Choosing the right device and dose matters more than marketing claims. A few practical guidelines from the red light therapy bone test and related experience:
- Prefer near-infrared when targeting deep tissues. If the goal is brain or deep joint penetration, 800–900 nm bands will reach further than 660 nm red.
- Use adequate output. Low-power wearables that emit only a few milliwatts at the skin are unlikely to deliver meaningful energy through thick bone. Panels and higher-output handhelds give better odds.
- Mind distance and geometry. Closer placement increases radiance exponentially. Pressing an emitter near the scalp or aiming through thinner cranial regions will increase delivered energy.
- Consider session length. If delivered power is low, increasing treatment duration raises total fluence. That can partially compensate for low transmission percentages.
Safety and Dosing Notes
More is not always better. There is evidence that overstimulating neural tissue or applying high fluence indiscriminately could be counterproductive for certain conditions. Some clinicians use modulation and targeted approaches to stimulate precise brain areas. Treating broadly with high-power devices requires caution and clinical guidance for serious neurological conditions.
Practical Takeaways from the Red Light Therapy Bone Test
- Light does penetrate bone. Even thick bone transmits measurable red and near-infrared photons, though most energy is attenuated.
- Near-infrared photons penetrate better than visible red. Expect a spectral shift toward NIR after passage through bone.
- Thickness, orientation, and anatomical windows matter. Transmission varies widely by location and alignment.
- Device output and proximity determine usable dose. Use devices with sufficient radiance and place them as close as is practical and safe.
- Small wearable LEDs may under-deliver. Gadgets that emit minimal power at the skin are less likely to reach deep tissues at therapeutic levels.
Ideas for Further Exploration
This red light therapy bone test was exploratory and not a controlled clinical experiment. It offers clear directions for more rigorous tests:
- Systematic mapping of transmission by exact skull location and thickness
- Comparison of multiple wavelengths and pulsed versus continuous emission
- Measurements using hydrated fresh bone and human cadaver skull samples for more clinically relevant data
- Correlating transmitted energy with measurable biological markers in tissue
Final Thoughts
Here is the practical takeaway: red and near-infrared light can reach tissues beneath bone, but a large portion of incident light is absorbed or scattered by the mineral and soft matrix. The red light therapy bone test establishes that penetration varies dramatically with wavelength, bone thickness, and geometry. For anyone targeting brain health or deep musculoskeletal problems, prioritize near-infrared wavelengths, choose devices with substantial output, and adjust dose and placement to account for attenuation.
If your goal is modest modulation of neural function, the small percentage that passes through bone could be biologically meaningful. If the goal is deep bone marrow therapy or treating a large joint, expect to need higher energies, longer sessions, or more powerful devices.
"Near-infrared wavelengths consistently out-perform visible red at penetrating bone and fatty tissues."
Repeat this mantra when comparing devices and planning treatments: wavelength matters, power matters, and anatomy matters. The red light therapy bone test gives a practical, measurable foundation to make those choices with more confidence.
Found This Interesting? Look At These Articles
🔴 The Red Light Therapy Facial Fat Loss Link: Myth Or Reality?
🔴 Does Red Light Therapy Help Scars? The Science
🔴 Red Light Therapy For Skin: Beauty Benefits, Potential Complications, And More
🔴 Psoriasis With Red Light Therapy: Potential Game-Changer?
Have You Seen These Reviews
🔴 Rouge G4 Pro Review: Most Advanced Red Light Panel Yet?
🔴 Best Red Light Panel Yet? Block Blue Light Mega Review
🔴 $800 Red Light Mask Has Lasers… But Why?
🔴 Omnilux Contour Mask Review: Still Worth It in 2025?
Alex's Bio
Alex Fergus wrote this blog post. Alex is an ISSN Sports Nutrition Specialist, Fitness Professional, and certified Superhuman Coach who continues to expand his knowledge base and help people worldwide with their health and wellness. Alex is recognized as the National Record Holder in Powerlifting and Indoor Rowing and has earned the title of the Australian National Natural Bodybuilding Champion. Having worked as a health coach and personal trainer for over a decade, Alex now researches all things health and wellness and shares his findings on this blog.