Updated: June 27 2026
Today, I'll discuss red light therapy for arthritis pain and the science and evidence on that topic. Red light therapy uses minimally heating minimally heating red and near-infrared light for a therapeutic effect.
In this blog post I'll explore the full science on what arthritis is, the needs for alternative treatments, and how red light therapy can work for inflammation and as a potential treatment. I'll be following the scientific consensus here - as I've got some informed opinions on my own that I will ignore in this blog post.
Next up, I discuss products. Most red light therapy at home for arthritis uses LED products, such as belts and wraps. But, most importantly, LED panels are used. And, just to be clear, I'm not considering laser light therapy here in great detail as it's generally more dangerous for consumers - so LEDs will have the main focus.
Let's begin:
Red Light Therapy For Arthritis Summary:
Right now, evidence is strongest for osteoarthritis, the most commonly ocurring arthritis type. Rheumatoid arthritis is less common and also responds well to red light therapy. Osteoarthritis is more local, rheumatoid arthritis is more systemic and has an autommune component.
The issue with arthritis is that current treatments can help but often don’t reverse the condition and may carry side effects.
For osteoarthritis, red and especially near-infrared (NIR) reduce pain and disability, even after light therapy treatment ends. NIR is more useful for deeper penetration. For rheumatoid arthritis, the evidence is more mixed but still suggests reduced pain, less morning stiffness, and better hand flexibility.
So far, so good! Research is growing exponentially in 2026 so this viewpoint will need to be updated in a few years' time.
As of 2026, pain measurements (the VAS scale) are lowered by 2-4 points on a 0-10 scale for osteoarthritis.
For home use, I recommend sufficiently powerful red and especially NIR devices, ideally larger panels for systemic effects. Targeted joint devices may help for localized problems are great as well. Red light therapy should be combined with exercise, sleep, diet, and other lifestyle strategies.
Best Devices (best at top):
1. Kineon MOVE+ - Use discount code AFERGUSMOVE - this device is best for the knee and other smaller joints
2. Chroma Ironforge - Use discount code ALEX - this device is recommended for bigger joints, such as the shoulders and hip.
3. Handheld Devices - any of the best/most reputable companies, such as Rouge, Mito Redm Block Blue Light, Mito Light EU, will do. This device is especially great for treating small joints, and getting a versatile device
4. A Wall or Body Panel - any of the best/most reputable companies, such as Rojo, Rouge, Block Blue Light, Mito Light EU, PlatinumLED, will do. This device is especially great for multiple joints and Rheumatoid Arthritis, which is a systemic condition.
Background Info Before Reading The Full Article:
The header picture above is AI-generated though.
If you need an introduction to what these terms mean, check the following resources:
- What Is Red Light Therapy?
- Red Light Therapy Explained: Basic Terms Guide
- Start Here - Light Therapy 101 & Buyers Guide
- Red Light Therapy Dosing Chart: The Raw Data From Hundreds Of Studies
- Red Light Therapy Dosing: Why It's Complicated!
- Red Light Therapy Wavelengths Benefits: The Ultimate Guide
- How Often Should You Use Red Light Therapy Explained
These resources should give you a basic understanding of how red light therapy works, and the discussions around it!
Understanding Arthritis: Basics Of Osteoarthritis, Rheumatoid Arthritis, And More
Having "arthritis" means having a joint disorder. Many different types of arthritis exist, but two of the most common types are osteoarthritis and rheumatoid arthritis. There's tons of clinical trials and other research published on these topics yearly.
I'll summarise some of the latest publications here (1; 2; 3; 4; 5; 6; 7; 8; 9; 10). And although acute joint pain is technically also included in arthritis, it's almost always chronic. Arthritis has affected most of your ancestors' lives, with cases being found in ancient Egyptian bones as well as prehistoric ones.
Over 100 different types of arthritis exist. Osteoarthritis - degeneration of the bone - is the most important one here. Osteoarthritis isn't characterized by high levels of (systemic) inflammation.
Next up, there are inflammatory types of inflammation, such as rheumatoid arthritis, ankylosing spondylitis, and others. The inflammatory types of arthritis can be caused in many different ways.
Viral infections can cause inflammatory arthritis, as do autoimmune processes (whereby the immune system attacks the body's own cells), as well as deposits that should't be there (e.g. in gout). And, sometimes the inflammatory arthritis is intertwined with health conditions, such as autoimmune conditions.
Let's explore osteoarthritis first though:
Osteoarthritis Basics
Osteoarthritis mainly affects you as you get older (2). One in three people is affected by osteoarthritis worldwide, with a higher percentage of women. A recent review study summarizes the predicament of osteoarthritis (OA) very clearly:
"The prevalence of OA is rising due, in part, to the increasing prevalence of OA risk factors, including obesity, physical inactivity, and joint injury. OA-related joint pain causes functional limitations, poor sleep, fatigue, depressed mood and loss of independence. Compared to age and sex-matched peers, OA patients incur higher out of pocket health-related expenditures and substantial costs due to lost productivity. Most people with OA (59-87%) have at least one other chronic condition, especially cardiometabolic conditions. Symptomatic OA may impair the ability of people with cardiometabolic conditions to exercise and lose weight, resulting in increased risk for poor outcomes. " (2).
So in a sense, the inactivity in modern society increases osteoarthritis risk, which then in turn makes it much harder to become active again. And, osteoarthritis makes your overall health go down because sleep and movement are negatively affected. Health care costs subsequently go up while maintaining your career can becomes harder.
Osteoarthritis also often affects joints you need for work, such as the hands, feet, knees, and hips (5). Obesity also increases osteoarthritis risk while making it harder to deal with, eventually. All tissues around the joint are affected, resulting in:
"pathologic changes in cartilage, bone, synovium, ligament, muscle, and periarticular fat, leading to joint dysfunction, pain, stiffness, functional limitation, and loss of valued activities, such as walking for exercise and dancing. " (5)
Current osteoarthritis treatment consists of physical exercise, dealing with being overweight or obese, steroid injections in the joint, stem cell therapy, and painkillers.
I'll come back to that topic in a second. Let's first help you understand inflammatory types of arthritis:
Inflammatory Arthritis: Rheumatoid Arthritis And More
Next up, there's inflammatory arthritis (3). Inflammatory arthritis comes with a few classic symptoms, such as swelling, redness, pain, degeneration, warmth, and loss of function. All of these symptoms are frequently but not always present in the most infamous type of inflammatory arthritis: rheumatoid arthritis.
Inflammatory more often has a systemic health (full-body) influence affecting it. Examples here are infections or autoimmune processes that didn't start in the affected joint itself.
Rheumatoid arthritis is even considered a full-blown autoimmune condition by itself, not just a joint disorder (6). A recent scientific review (that integrates previous research) states that rheumatoid arthritis is:
"caused in many cases by the interaction between genes and environmental factors, including tobacco, that primarily involves synovial joints. It typically starts in small peripheral joints, is usually symmetric, and progresses to involve proximal joints if left untreated. Joint inflammation over time leads to the destruction of the joint with loss of cartilage and bone erosions. " (6).
So, as one famous physician I know would say: "genetics loads the bullet, and environment and lifestyle pull the trigger". Rheumatoid arthritis is hard to diagnose, initially though, due to the absence of good testing. Once the disease progresses, however, clinical symptoms become undeniable.
Prescription drugs are the primary current intervention for rheumatoid arthritis. Lifestyle changes such as exercise and supplements may also help but often don't prevent the deterioration of the joints over time. Management of rheumatoid arthritis has become better over the years, though, through new drug interventions, but the condition is not curable nor reversible (9).
In developed nations, about 0.5% of the population is affected by rheumatoid arthritis (10). People in cities are slightly more affected than in rural areas.
Moving on:
Other Arthritis Types
Next to the two main arthritis types, many other types exist as well, such as psoriatic arthritis, reactive arthritis, and gout (4; 8; 11; 12; 13). I won't explore these options further, although future articles will consider them in great detail.
The Need for Alternative Methods to Treat Arthritis

At the most fundamental level, the biggest problem with treating arthritis is that there's often no cure, according to the scientific consensus in medicine. That's especially the case with osteoarthritis and rheumatoid arthritis.
Osteoarthritis Treatment & Side Effects
So let's consider the current gold standard of osteoarthritis treatments and its problems. Tons of publications emerge yearly on this topic - I'll explore the latest evidence here (14; 15; 16; 17; 18; 19).
New drugs have been developed to counter osteoarthritis, for instance, such as "disease-modifying osteoarthritis drugs" (DMODs), but these don't have long term data behind them and potential future risks are also unknown.
Next up, platelet-rich plasma and stem cell injections have been extremely promising in the last decade. Individualized treatments for different types of osteoarthritis may also help.
The simplest options, however, are still weight loss, physical therapy, and exercise. These options generally decrease pain, help people function better, and improve their quality of life. The cartilage that has been damaged, however, doesn't regenerate with those options.
And then there are painkillers with long-term risk, especially for people with heart disease. Injections may improve pain but risk deteriorating the joint even further. And some painkillers are addictive and, therefore, not the best option.
So we're at an impasse - nothing fundamentally fixes or reverses osteoarthritis. A similar trend is true for rheumatoid arthritis:
Rheumatoid Arthritis Treatment & Side Effects
Rheumatoid arthritis is generally more complex than osteoarthritis because of the autoimmune component. Treatments, once again, exist but slow down the progression and manage it instead of reversing it (20; 21; 22; 23; 24).
New pharmaceutical strategies have improved the course of rheumatoid arthritis, especially with early treatment. Early treatment prevents the destruction of the joints, and therefore a damaging feedback loop of poorer joints, more pain, and more treatments.
Through pharmaceutical means and early treatment, remission can be achieved where the condition's intensity remains very low. Nevertheless, treatments are primarily pharmaceutical in nature and thus often paired with side effects.
For instance, a class of anti-rheumatic drugs called "Disease Modifying Anti Rheumatic Drugs" (DMARDs), have potential side effects such as liver problems, gut and digestive dysfunction, nausea, changes in allergies, loss of appetite, and more.
So even in case of rheumatoid arthritis, there's need for alternative treatment options.
A recent review states the following about rheumatoid arthritis factors that aren't always targeted:
,
"Environmental factors, such as diet and cigarette smoke, may influence susceptibility to autoimmune diseases and interfere with inflammatory pathways. Mediterranean diet, low salt intake, cocoa, curcumin, and physical activity seem to show beneficial effects, however studies of dose finding, safety and efficacy in [Rheumatoid Arthritis] need to be performed." (24)
So, currently available options are promising, albeit need more scientific validation.
Next up, I'll explore the science on the question of "Does red light therapy actually work for arthritis?" Let's go:
So, Does Red Light Therapy Actually Work for Arthritis?

First, let me take a little detour. Red light therapy uses minimally-heating red and near-infrared light for healing purposes. Red light is visible to the human eye while near infrared light isn't.
Both of these light types penetrate into your tissue and have biological effects there. I recommend reading the What Is Red Light Therapy guide if you want to learn more about the basics.
There's quite a lot of science on the topic of red light therapy and arthritis. I'll start with red light therapy for pain in general - which is an extremely frequent problem with arthritis:
The Massive Red Light Therapy Benefits For Pain
Red light therapy - or called "photobiomodulation or "low level laser therapy (LLLT)" in medicine - has tons of different effects for different types of pain (25; 26; 27; 28; 29; 30; 31; 32; 33; 34).
There's an effect for both acute and chronic pain. In most cases, if there's chronic inflammation, that's affected too positively. Many different types of acute and chronic pain are affected, such as lower back and neck pain, musculoskeletal pain, neuropathic pain (in the nerves), fibromyalgia, oral pain such as in dentistry, tendon injuries, myofascial pain and other types.
The different types of pain affected by red light therapy are almost too countless to mention. Generally, for pain, you'll need a higher dose of red light therapy because the light is stimulatory at medium or optimal levels, and at even higher levels, it inhibits. That inhibitory process is great for countering pain.
The levels of evidence vary for different types of pain though - for musculoskeletal pain or tendon injuries, there's lots of evidence. For other types of pain, such as after a traumatic brain injury or neuropathic pain, the evidence is a little bit less strong.
Nevertheless, the fact that the side-effect-free red light therapy counters chronic pain offers tons of perspective. Red light therapy functions as a local nerve block at a very high dose, thereby stopping all sensation of the pain in many cases.
That pain relief can last for hours and even days. The topic is highly complex, though, as the device that's applied matters, whether LEDs or lasers are used, the power output and distance used, wavelengths, etcetera. I won't go into detail here, the only thing you have to remember is that red light therapy is very promising for dealing with pain.
Next up, let's zoom in on the topic we're talking about today:
Red Light Therapy For Joint Pain
Next up, there's red light therapy for joint pain specifically. In many different studies, red light therapy reduces pain, improves blood flow, enhances joint mobility, and more (35; 36; 37; 38; 39; 40). Here you can see the difference in pain between
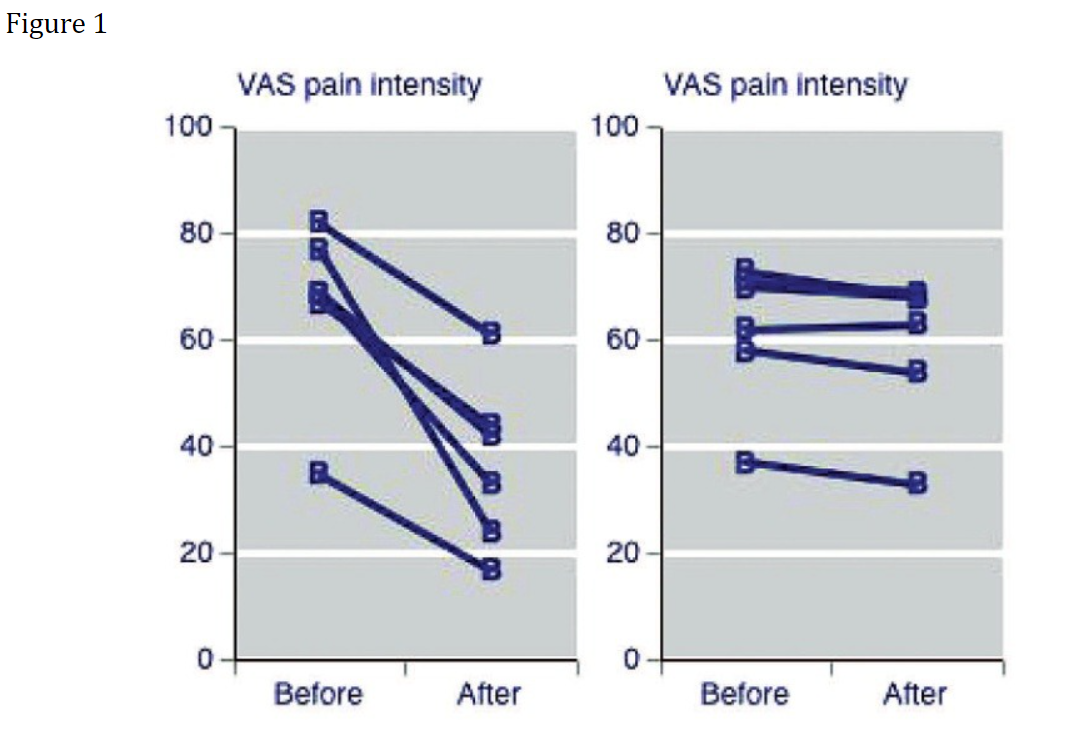
These results occurred after treating several times per week for a period of up to four weeks in different studies.
Usually, though, you need to follow common sense advice. For instance, when you're using red light therapy, you can't just continue with your normal life without making any changes. With a joint injury, you'll often have to move, but not too much.
Benefits are found for many cases, such as ankle and foot problems, non-specific lower back pain and non-specific neck pain. Non-specific here means that no underlying physiological issue could be identified, but people still experienced pain and limited functionality in their daily lives.
Next up:
Red Light Therapy For Osteoarthritis
Many different review studies have been published on red light therapy for osteoarthritis (35; 36; 37; 38; 39; 40; 41; 42; 43; 44). I'm citing reviews here as there are dozens of individual studies on red light therapy for osteoarthritis, which are too many to cover here.
Most of these reviews have been carried out on the knee. In general, most reviews tended to be neutral in the early to mid-2010s, not showing much benefit. But, in the last few years, the tides have turned and there is a benefit of using red light therapy for osteoarthritis.
The near-infrared wavelengths do better in most studies. So, if you had to choose between red and near-infrared, I'd opt for the latter.
For nerds, the results section of a recent study states the following:
22 trials (n=1063) were meta-analysed. Risk of bias was insignificant. Overall, pain was significantly reduced by LLLT compared with placebo at the end of therapy (14.23 mm Visual Analogue Scale (VAS; 95% CI 7.31 to 21.14)) and during follow-ups 1-12 weeks later (15.92 mm VAS (95% CI 6.47 to 25.37)). The subgroup analysis revealed that pain was significantly reduced by the recommended LLLT doses compared with placebo at the end of therapy (18.71 mm (95% CI 9.42 to 27.99)) and during follow-ups 2-12 weeks after the end of therapy (23.23 mm VAS (95% CI 10.60 to 35.86)). The pain reduction from the recommended LLLT doses peaked during follow-ups 2-4 weeks after the end of therapy (31.87 mm VAS significantly beyond placebo (95% CI 18.18 to 45.56)). Disability was also statistically significantly reduced by LLLT. No adverse events were reported. (35)
So what does this mean, in plain English? Both pain and disability are reduced. Pain reductions continue after therapy is stopped, peaking two to four weeks later.
Also, pain reductions are 31.87 millimeters on a "Visual Analogue Scale" (VAS) that measures pain from zero to ten in centimeters. "Zero" here stands for no pain at all and "ten" for the worst imaginable pain.
You can imagine that a reduction in pain of more than three centimeters is extremely significant and life-changing for many people.
Recommended wavelengths range from the high 700 nanometers (nm) to the low 900s. Other studies recommend the 600 - 1,000 nanometer range.
Many different mechanisms are proposed that explain why there is such a pain reduction with red light therapy for osteoarthritis. For instance, fibroblast regenerate, which support connective tissue. Energy production increases. Oxidative stress is lowered, which is often a byproduct of excess stress. Edema and hemmorrhages, if present, are impeded. And, overall, there's not just a painkilling effect but also an anti-inflammatory effect.
Of course, the astute reader will notice that these mechanisms - pain killing and countering inflammation - overlap with many pharmaceutical drugs used for osteoarthritis.
Nevertheless, a big problem in the research on using red light therapy for osteoarthritis is that there's no standarization. Treatment methods, such as whether the joint or the nerve is treated, the wavelengths used, the reporting of the treatment protocols, and the exact dosage, differ and are sometimes not optimal. Therefore, at least some studies don't show results.
Also, combining red light therapy with an exercise program may yield superior results (41). That statement should be a bit common sense but I'd mention it anyway.
The same is true for sleep and osteoarthritis, for instance, where poor sleep doesn't just impede the function the next day while making the pain worse, but may play a causal role as well (45; 46; 47). Also, while less common sense, curcumin also has a significant impact on osteoarthritis, lowering pain and improving function (48; 49; 50). My point here is that you shouldn't bet on a single horse.
Next up, let's move on to osteoarthritis:
Red Light Therapy For Rheumatoid Arthritis
Then there's red light therapy for rheumatoid arthritis (51; 52; 53; 54; 55).
Here's one outcome of a review study that I'll break down into plain English in a second:
A total of 222 patients were included in the five placebo-controlled trials, with 130 randomized to laser therapy. Relative to a separate control group, LLLT reduced pain by 1.10 points (95% CI: 1.82, 0.39) on visual analogue scale relative to placebo, reduced morning stiffness duration by 27.5 minutes (95%CI: 2.9 to 52 minutes) and increased tip to palm flexibility by 1.3 cm (95% CI: 0.8 to 1.7). Other outcomes such as functional assessment, range of motion and local swelling did not differ between groups. There were no significant differences between subgroups based on LLLT dosage, wavelength, site of application or treatment length. For RA, relative to a control group using the opposite hand, there was no difference observed between the control and treatment hand for morning stiffness duration, and also no significant improvement in pain relief RR 13.00 (95% CI: 0.79 to 214.06). However, only one study was included as using the contralateral limb as control. (53).
So, "Low Level Laser Therapy" (LLLT) reduced the total pain by 11% on average. Morning stiffness was reduced while the range of motion in the wrist (which is often affected) was enhanced. Swelling didn't change though.
Dosage, wavelength, and treatment time, weirdly enough, didn't matter too much here (so far!). Nevertheless, other review studies do confirm this outcome, showing benefits for pain, quality of life, and functionality across the board. And, as with osteoarthritis, the reporting about the treatment protocols isn't always perfect in scientific studies - which is true across the entire red light therapy literature.
For the best outcomes though, you'll have to combine red light therapy for rheumatoid arthritis with other lifestyle interventions. As almost always, there's a range of interventions that will help with a health condition, not just one.
Red Light Therapy Hip Pain
Hip pain can have many causes. One common cause is hip osteoarthritis but many others exist as well. Hip fractures are an example, or, a "new hip" after surgery for osteoarthritis, for instance.
Not too many studies can be found on red light therapy for hip pain, let alone reviews that integrate previous research on the topic (56; 57; 58; 59; 60). Generally, here, red light therapy for hip pain improves functionality while reducing pain. Frequently, whenever it's possible, the combination of exercise and red light therapy is superior to either alone.
Red light therapy may even speed up the healing process after fractures, although more research is needed here for its effects on different stages. And, after a hip replacement ("hip arthroplasty"), red light therapy lowers pain while lowering inflammation. The researchers studying red light therapy after a hip replacement write:
The study consisted of 18 post-surgical hip arthroplasty patients divided into two groups (n = 9 each) placebo and active PBMt ["Photobiomodulation"] who received one of the treatments in a period from 8 to 12 h following THA surgery. PBMt (active or placebo) was applied using a device consisting of nine diodes (one super-pulsed laser of 905 nm, four infrared LEDs of 875 nm, and four red LEDs 640 nm, 40.3 J per point) applied to 5 points along the incision. Visual analog scale (VAS) and blood samples for analysis of the levels of the cytokines TNF-α, IL-6, and IL-8 were recorded before and after PBMt application. The values for the visual analog scale as well as those in the analysis of TNF-α and IL-8 serum levels decreased in the active PBMt group compared to placebo-control group (p < 0.05). No decrease was observed for IL-6 levels. We conclude that PBMt is effective in decreasing pain intensity and post-surgery inflammation in patients receiving total hip arthroplasty.
So, a combination of red and near-infrared works in this case, but there's little comparison available right now. Overall, the results of red light therapy for hip pain and functionality are positive but a lot more research is needed here.
Let's consider the knee next:
Red Light Therapy Knee Pain

Knee pain has different causes. Sports injuries, such as torn ligaments, can cause knee problems over time, as well as cartilage problems. And, the knee is one of the most common places people develop osteoarthritis over time. I won't go into osteoarthritis too much in this section, but red light therapy for knee pain in general instead.
So here's the outcome:
- In many studies, red light therapy can enhance the healing of knee ligaments, such as the medial collateral ligament or anterior cruciate ligament (61; 62; 63; 64; 65; 66). These conclusions are based on animal studies, however. Stiffness, inflammation, and healing speed improve while the risk of joint damage decreases. Over time, the tensile strength of the ligaments also improves. If you didn't know, ligaments hold bones together and offer stability to joints.
- Next up, red light therapy for the knee meniscus shows benefits as well (68; 69; 70). In this case, some human research is available although it's limited. There are significant improvements in symptoms though, and red light therapy may be recommended as a preliminary step for people who wish to avoid meniscal surgery.
- Overall, red light therapy for the patella tendon is also promising, although more research is needed once more (71; 72; 73). There's likely a very good effect here because red light therapy speeds up tendon repair.
So in a wide variety of knee-related problems, red light therapy likely helps. Next up:
Red Light Therapy Shoulder Pain
The term "shoulder pain" is just as problematic as "knee pain", as there can be many different causes. Tons of different shoulder pathologies exist, such as a frozen shoulder, rotator cuff problems, bursitis, shoulder osteoarthritis, supraspinatus impingement, rheumatoid arthritis of the shoulder, and so forth.
I won't venture too deeply in any of these pathologies but look more broadly at the research of red light therapy for the shoulder. Lots of research is available on this topic though, that I will go through (74; 75; 76; 77; 78; 79; 80; 81; 82; 83). Generally, once again, red light therapy works best when combined with exercise therapy.
- For a shoulder tendon problem, red light therapy can lower pain as much as two points on a zero to ten VAS scale (74).
- Disability, pain, and functional assessment don't improve significantly in a shoulder impingement syndrome - where the supraspinatus muscle of the shoulder is affected - using red light therapy (75). Another study draws the opposite conclusion, showing improvements in pain, functionality, and medication intake (76).
- In case of a frozen shoulder, likely positive effects exist as well (77).
- Overall, red light therapy could play a supportive role in shoulder rehabilitation in general (79). There's little to no risk in trying red light therapy, and only upside.
- Studies aren't all positive. In shoulder and neck girdle problems, red light therapy didn't outperform placebo (80). In case of painful adhesive capsulitis in the elderly, however, extremely positive results are found (81).
- Most protocols use treatment times of four to twelve weeks, with two to three weekly sessions.
- And, as always, you can't be 100% sure about the outcomes of the results because almost all red light therapy studies don't have standardized reporting.
Overall, though, red light therapy for shoulder pain is decently positive, but more high-quality human research is needed.
Red Light Therapy For Arthritic Hands

There's a surprising amount of research available on red light therapy for arthritis hands (84; 85; 86; 87; 88; 89; 90).
- In osteoarthritis of the hands, red light therapy can improve the range of motion (84).
- In Bouchard's and Heberden's osteoarthritis, where bony deformations exist, pain decreases significantly while the range of motion of the joints increases (85). There's an extremely strong effect here.
- Methodological quality of the studies, in this case, can be low again, as researchers don't always have full understanding of dosing parameters, or might not report them (86). That problem likely leads to the absence of effects in some studies, as researchers might overdose or might treat an area too small, or for other reasons (87; 88).
- In rheumatoid arthritis for the hands, red light therapy might not work though (88). At least, so far
So, overall, regarding red light therapy for arthritis hands, there's more evidence for osteoarthritis than rheumatoid arthritis.
Moving on:
The Effects of Red Light Therapy on Inflammation
Swelling, inflammation, the immune system, and oxidative stress are all interrelated concepts. But how these all interrelate is often an enigma for the average person. The oversimplified version is this: inflammation is an immune system reaction that's intertwined with oxidative stress. And swelling is a frequent side-effect of inflammation.
I'll get to the topic of swelling in a second. First up, the research on red light therapy and inflammation (89; 90; 91; 92; 93; 94; 95; 96). In many different situations, red light therapy normalizes inflammation levels. That's helpful, as some inflammation is healthy but excess, chronic inflammation becomes damaging to the body (97; 98; 99; 100).
Chronic inflammation is intertwined with many modern diseases, such as diabetes, heart disease, neurological illnesses, and so forth. Inflammation isn't bad though - you need inflammation as part of a repair mechanism. So if you fall on your knees, the resulting inflammatory response is a good thing.
Normally, that inflammation subsides and life goes on. But if you're inflamed 24/7, it becomes a problem. Fortunately, chronic inflammation is one area where red light therapy can specifically help. And by countering chronic inflammation, overall health improves.
In many different cases, such as wound healing, microbe infections, organ problems, joint injuries, and more, inflammation levels improve over the long run with red light therapy.
Now here's why this argument on inflammation matters: even osteoarthritis is characterized by inflammation, current research claims (101; 102; 103; 104). And, the inflammation is a lot more obvious in other arthritis conditions such as rheumatoid arthritis (105; 106; 107; 108).
Theoretically, red light therapy should help a lot in the area of inflammation for both osteoarthritis and rheumatoid arthritis. And, in many of the studies on both conditions, there is an effect on inflammation. So overall, the red light therapy effects on inflammation aid osteoarthritis and rheumatoid arthritis too.
Next up, let's consider another important topic:
Red Light Therapy For Swelling
In many different cases, red light therapy for swelling works (109; 110; 111; 112; 113; 114). However, just as is the case with inflammation, I'd like to see more direct studies on this. It's very likely though, that because red light therapy affects so many domains of arthritis, the swelling (edema) is affected too.
The Future of Arthritis Treatment and Red Light Therapy
Current research on red light therapy for arthritis treatment is extremely promising. There's lots of evidence for pain, daily functioning, muscle and bone strength, and so forth.
The only thing that's necessary on the future of arthritis treatment and red light therapy are longer-term studies and more specific studies. These specific studies include topics such as how red light therapy influences inflamamtion and swelling directly, and the effects of that on the condition.
And, I'd be very interested in other wavelengths of light, such as green and amber, which have pain-killing effects and anti-inflammatory effects in some cases too. Nevertheless, the future is bright!
Red Light Therapy At Home For Arthritis
So, what are the recommendations for red light therapy at home for arthritis? You can analyze this topic at several levels, which I'll subsequently explore below.
First up, you'll want a product that has sufficient power output. A higher powered product allows for deeper penetration, which means a better therapeutic effect. More power output directly leads to deeper penetration, so you don't want a low-powered device.
That power output is especially important for some joints, such as the knee, the hip, the shoulder joint, of which many parts are located deeper below the skin. For some joints, such as the wrist or hands, you can use a lower-powered device. The counterargument there is that the treatment will be suboptimal as you're not getting the benefits of a systemic approach.
Which leads me to my next point:
Secondly, you'll want a product that treats large areas of the body. Ideally, you'll want a full-body setup but that's expensive. But, bigger areas that are treated are generally better.
And, in case of rheumatoid arthritis, you'll probably want to follow a full-body approach as much as possible. In case of osteoarthritis, assuming you only have a localized problem, you can get away with targeted treatment.
But, keep in mind that even with osteoarthritis, there's often not just one issue at one joint, but there often are comorbidities like diabetes or heart disease, people are more frequently overweight, and so forth, all of which red light therapy can help with. Red light therapy even helps workout recovery and performance, which in turn can be a huge boost for helping people slow down osteoarthritis or deal with its symptoms. Check out the video on red light therapy and workouts if you're interested.
Thirdly, you'll want a red light therapy product that emits both red and near-infrared light. Both parts of the light spectrum have independent benefits but the near infrared is especially promising for arthritis because it penetrates deeper.
Hence, below I'll offer you a few great options for red light therapy at home for arthritis, focusing on bigger panels:

Again, there are several reasons you'll want a bigger red light therapy panel for arthritis.
- First up, the inflammation is systemic across the body with many types of arthritis, such as osteoarthritis and rheumatoid arthritis.
- Secondly, treating your entire body allows you to recover faster, which helps you keep moving, which in turn helps deal with the arthritis symptoms across the board.
- Thirdly, red light therapy helps many areas that are affected by arthritis, such as sleep quality, the need for recovery, fat loss, and building muscle, all of which generally become harder with many different arthritis forms!
So, if you can opt for a red light therapy panel, do it.
Now, you may ask, why not choose for a belt or a wrap or another type of red light therapy product. Usually, these products don't have the best power output and/or they don't treat bigger areas of the body. Hence, I don't recommend these options as a main course for arthritis.
Lastly, there's an honorable mention that's extremely important for arthritis in general, because it offers the most excellent spot treatment currently available. That's the Kineon Move+. You can read the article by Alex Fergus of that device below:

The reason I recommend this device so strongly is because it's specifically made for the joints. The Move+ can target the joints in a way regular panels cannot do, as it's directly placed on the skin for deeper penetration, as well as including pulsing with the same goal.
And, as of 2026, I consider the Chroma Ironforge a great option for arthritis:

2026 Update: Arthritis Course Episode
In 2026, I'll be publishing an update on the topic of light therapy for arthritis. You can access that course for free HERE:
If you don't want to see that full episode on red light therapy for arthritis, then, consider my full notes below, of my conclusion, updated to the 2026 science:
- Red light therapy is great overall pain-lowering-effect for osteoarthritis, that translates into better function
- VAS scale outcoomes - which measure subjective levels of pain - lowered by 2-4 points (0-10 scale)
- Better stiffness levels and lower disability as well in many studies.
- Most research out there is still on knee osteoarthritis.
- The mechanism is changes in the immune system and inflammation, and boosting circulation and tissue regeneration, thereby giving you improvements across the board
- Light therapy is still best combined with different therapies, such as hydrotherapy and exercise.
- High intensity treatment better in some reviews. Therefore: contact method and higher power
- NIR better in some reviews (808 - 1,070nm)
- And yet, we still have many unknowns around dosing (wavelength, J/cm2, treatment area, device)
- Doses of up to 12 J/cm2 best, but arguably up to 30 J/cm2
- Some thermal effects may improve outcomes!
- Frequent treatment better, so maybe aim for 4-5 times weekly.
- Results can last for months after a treatment period
Also, if you're curious about many of the other benefits and goals to pursue with red light therapy, consider my science tool here:

Conclusion: Red Light Therapy For Arthritis Is Extremely Promising
Hopefully, you're convinced that red light therapy for arthritis is extremely helpful. And, not only is pain reduced in conditions such as osteoarthritis and rheumatoid arthritis, but function, inflammation, and quality of life also get better.
For decent results, use a targeted red light therapy at home for arthritis device, such as a tabletop panel. Then treat the joints affected by arthritis with that. For the best results, however, full-body treatments are recommended because these affect the underlying systemic inflammation that plays a role in the most important arthritis cases.
This is a post by Bart Wolbers. Bart finished degrees in Physical Therapy (B), Philosophy (BA and MA), Philosophy of Science and Technology (MS - with distinction), and Clinical Health Science (MS), has had training in functional medicine, and is currently chief science writer at Lighttherapyinsiders.com
Found This Interesting? Then You Might Like:
- Start Here - Light Therapy 101 & Buyers Guide
- What Is Red Light Therapy?
- Science Tool: Simplifying Routines, Benefits & Device Selection
- Kineon Move+ Pro Review: Targeted Red Light For Joints?
- Discount Codes, Deals & Recommendations - Red Light Therapy
- How To Use Red Light Therapy At Home: Expert Tips
- 36 Powerful Red Light Therapy Benefits
- James Carroll Photobiomodulation Course: 16 Amazing Lessons Learnt